







Weekly Checkup
June 21, 2024
Is Curing Hepatitis C a Budget-friendly Solution for Medicaid?
Last week the Congressional Budget Office (CBO) released a report, “Budgetary Effects of Policies That Would Increase Hepatitis C Treatment,” which analyzes the larger financial impact of enacting policies to treat and subsequently cure Hepatitis C (HCV) within the Medicaid population. Let’s dive into the report to better understand CBO’s findings and why this cure-directed treatment program could lower total government spending in the long run.
First, let’s talk about HCV. HCV is one of five strains of the hepatitis virus, a pathogen that targets the liver causing inflammation and, over prolonged periods, irreversible liver damage. As a bloodborne virus, HCV is spread when infected blood enters another uninfected body, primarily by the sharing of needles for injectable drug use. Among the five strains, HVC is considered the deadliest, with 70 percent of people suffering from chronic HCV developing liver disease and a further 20 percent developing cirrhosis (a severe form of liver scarring). Per the Department of Health and Human Services, HCV is the most prevalent form of hepatitis in the United States with an estimated 2.5 million to 4.7 million Americans afflicted. Even more troubling, of those actively infected with chronic HCV, as many as 75 percent remain unaware of their infected status until the onset of more serious complications.
Next, let’s discuss direct acting antivirals (DAA), which are an HCV treatment that work by blocking the action of essential proteins, preventing the further replication of HCV within the host. Prior to the introduction of DAAs, HCV was very challenging to treat, but following their approval in 2013, HCV became a curable disease practically overnight. DAAs are broadly effective, work in a few weeks, and have minimal if any side effects. Unfortunately, however, they come at a steep price. At a little over $24,000 on average per individual treatment course, the high cost of DAA treatment has made some state Medicaid programs reluctant to completely cover the drugs. But in a recent Journal of the American Medical Association (JAMA) study, researchers contended that this reluctance resulted in a slower uptake of these highly effective DAA treatments among Medicaid recipients, and that loosening sobriety restrictions of DAAs may improve access to HCV treatment.
In its analysis, CBO focused on two sample policies that “would increase treatment rates among Medicaid enrollees and thereby affect federal spending on healthcare.” Of note, CBO found that “savings from health care costs that would be avoided by increased hepatitis C treatment would more than offset direct spending on that treatment.” In other words, CBO contends that while DAA treatments have a high upfront cost, in the long term, the cost to cure HCV is significantly cheaper than covering the prolonged complication costs associated with HCV–infected Medicaid enrollees. By CBO’s estimation, assuming Medicaid enrollee uptake of DAAs increased by roughly 10 percent, Medicaid subsequently would save approximately $700 million in total HCV complication spending, while only spending roughly $500 million on testing and DAAs. This equates to a reduction in spending of about $200 million over the following 10 years.
It seems there’s some promising evidence that curing HCV is cheaper than treating its symptoms, and should Medicaid more broadly cover the cost of DAA treatment courses – thereby increasing the Medicaid population’s uptake of DAAs – Medicaid could even save a little money. Notably, for DAA uptake to accurately decrease total spending within the HCV-affected Medicaid population, increased outreach and implementation of the DAA treatment program is necessary to improve testing, treatment, and adherence rates. An important point of consideration: CBO estimates cannot account for the unpredictable lifestyle choices of many of the Medicaid enrollees afflicted by HCV that can lead enrollees to wander off their coverage, resulting in a less-than-accurate savings projection. Nevertheless, CBO’s findings suggest policymakers should keep an open mind to the possibility of loosening restrictions to DAAs for HCV.
CHART REVIEW: Highlights of Recent Health Care Job Growth
Henry Roberts, Health Care Policy Intern
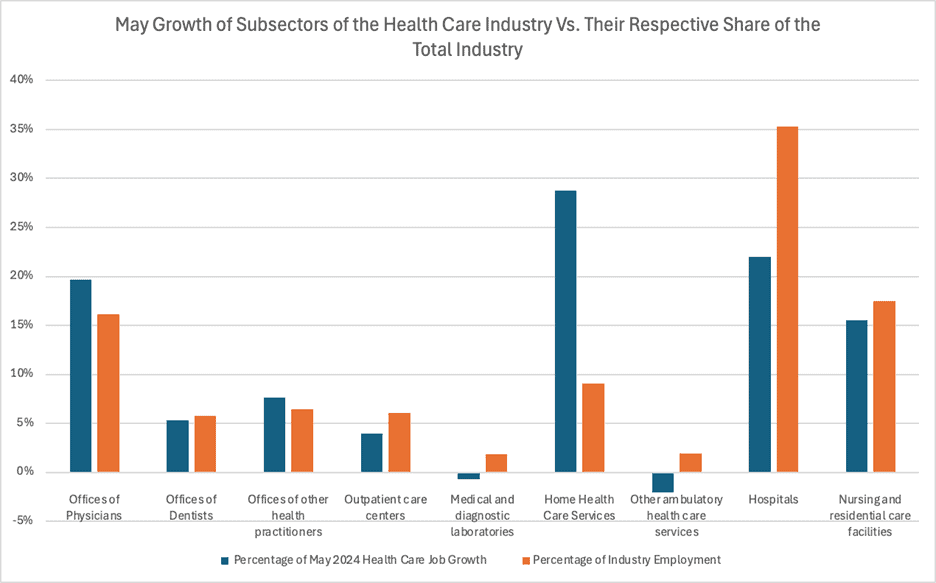
Last month, the health care industry added a total of 68,300 jobs, reaffirming its position as one of the top sectors for employment gains. The source of this growth came from a variety of subsectors within the industry. Most segments of the health care sector experienced growth rates similar to their respective share of the industry. This is indicated by a similar height of the blue and orange lines – representing May growth and the subsector’s share of industry employment, respectively – in the chart below. A few segments deviated significantly from this trend, however.
Among these subsectors was home health service employment, which accounted for 29 percent of the new jobs despite only making up 9 percent of the overall industry. The primary drivers of this growth are an aging population and favorable traditional Medicare reimbursement for home medical services. The Bureau of Labor and Statistics (BLS) anticipates that employment in this area will rise 22 percent by 2032.
Also noteworthy, hospital employment grew significantly below its share of the sector, accounting for 22 percent of growth while making up 35 percent of the industry. Since this is just a single month’s job data, it is not necessarily representative of long-term industry trends. For example, hospital margins overall are performing much better than in previous years, with an average of 2.3 percent as of December 2023. Margins had reached a low of –3.3 percent on average through January and February of 2022. Thus, the relatively faster growth in hospital employment is not surprising.
Other noteworthy changes are a slight decrease in employment within medical and diagnostic labs and “other ambulatory health care services.” BLS includes ambulance services in this category, which account for roughly half of the jobs within this group.
Sources:
https://www.bls.gov/news.release/pdf/empsit.pdf
https://www.bls.gov/ooh/healthcare/home-health-aides-and-personal-care-aides.htm#tab-6
https://www.grandviewresearch.com/industry-analysis/us-home-healthcare-market-report
