







Weekly Checkup
November 8, 2024
The Moving Target of Health Policy
Talking about health policy in public can be very frustrating. Not as frustrating as being a Pirates fan or a deficit hawk, but frustrating. One reason is that there is no such thing as “health care.” There are a million different kinds of health care, ranging from acute care in response to cardiac arrest to elective procedures for cosmetic, or other goals. It is a lot easier, for example, to argue that one ought to let market forces dictate the availability and pricing of the latter than the former. Dislodging the public – and, especially, the press – from the notion that there is a single, life-or-death health care that must be free and universally available is a constant challenge.
It is also true that there is no such thing as “the patient.” The population looks different in different geographies across the United States and the population’s health needs differ along with that. At the same time, the population changes over time – the aging of the population along with the baby boom generation is the most visible example – and the kinds of therapies, drugs, and devices that are most useful change right along with it.
Consider the chart (below). In 2000, 55 percent of the adult population had no chronic diseases, yet only 10 years later this had fallen to just below 50 percent. Over the ensuing 10 years, however, the fraction barely budged. The flip side is that the number of people with two or more chronic conditions rose in a mirror-image fashion.
Recognizing that the future will contain similar disease dynamics should influence the design of health payment systems, particularly Medicare. At one end of the extreme is fee-for-service medicine characterized by traditional Medicare. If you treat a senior for diabetes, you get the standard diabetes visit fee. If you treat chronic kidney disease, the provider gets a different fee – and similarly for congestive heart failure.
But suppose the patient shows up with congestive heart failure and diabetes. Do I just order from health care entrees off the fee-for-service menu? What if all three conditions are present? The patients are complicated, and the right care is unlikely to cost the same as adding up the individual visits.
At the other end of the spectrum is a flexible model that pays for the quality of outcomes. Or, if health outcomes are hard to measure – as they usually are – pay a single lump sum based on the health of the patient; i.e., a risk-adjusted amount. This permits the provider to choose the mix of treatments instead of a fee-for-service model dictating the approach. And it provides the care team an incentive to do this in as cost-efficient a fashion as possible.
The flexibility to adapt to the care needs of changing populations is one reason to favor moving Medicare toward a model based on Medicare Advantage – and move it away from traditional Medicare as fast as possible. It makes no sense to tie the insurance system for seniors to the practice patterns and health conditions of history instead of adapting to their current needs.
Chart by Parth Dahima, Health Care Data Analyst
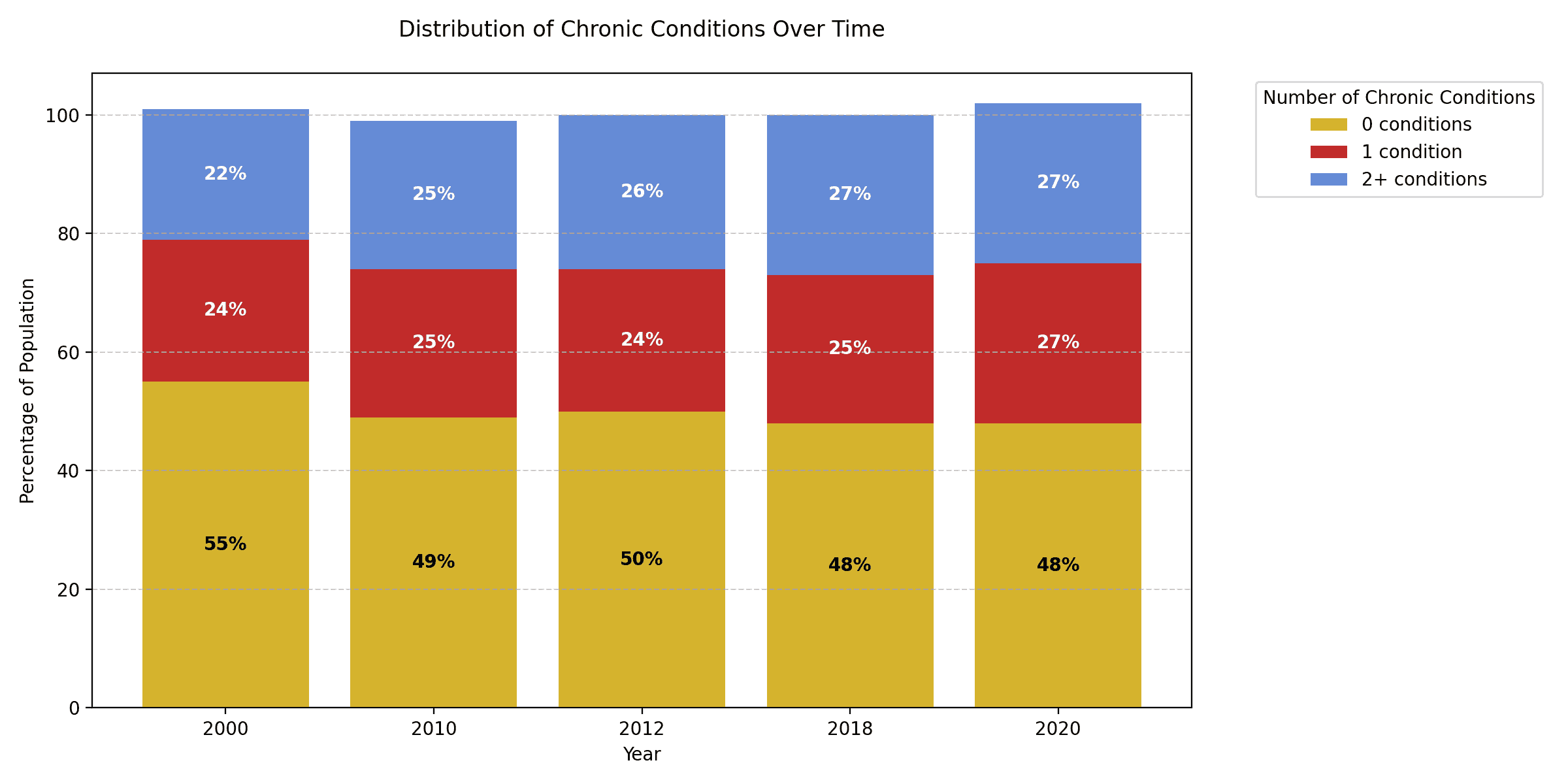
Sources: American Public Health Association and Centers for Disease Control and Prevention
