







Weekly Checkup
April 19, 2019
Price Transparency and Market Competition
Earlier this year, the Department of Health and Human Services proposed a rule that, among other things, requested comment from the public on whether hospitals and physicians should be required to publish their negotiated rates with insurers. While the question hasn’t garnered much attention, the proposal could have far-reaching implications for America’s health care system.
Broadly speaking, transparency is a good thing, especially in complicated transactions involving expensive goods or services. Even in uncomplicated transactions, knowing the various prices facilitates an effective marketplace. My wife and I recently needed to replace the driver-side mirror on my car, so we obtained several estimates for parts and labor before determining that duct tape is pretty cost effective. Yet why don’t patients have access to the same kind of price data? If patients could shop for medical services based on price and quality, wouldn’t that foster competition and bring down health care costs? Perhaps, but the answer is a lot more complicated than that.
Very few of us pay directly for our health care. If you have insurance, there is an intermediary between you and the provider. Yes, there are deductibles, copays, and coinsurance, but that intermediary typically affects the price you pay. For example: I have very basic dental insurance, and while it doesn’t cover much, it does limit what my dentist is allowed to charge me. My dental insurance provider has negotiated certain rates for certain services with certain providers. If I change insurers, I might find that my dentist is suddenly charging me an entirely different price for the same service.
The problem with transparency, as a result, is that there is no single price. A hospital may have 10 different prices for 10 different insurers all for the same procedure. The Trump Administration is floating the idea of requiring all the prices negotiated between providers—hospitals, physicians, etc.—and insurers to be available publicly. I’m not sure how helpful this transparency would be. On the one hand, as a consumer, knowing the different prices doesn’t really help me, because I can still only go to the providers in my network to get the negotiated prices, and I’m still going to pay the same negotiated rate regardless of what other insurers have negotiated. Over the course of several years, I might be able to jump between insurers to get the best prices, but the prices are likely to be renegotiated more frequently than I change insurers anyway.
On the other hand, there is real danger to the market when insurer A finds out that insurer B is paying $4,000 less for a procedure and demands the same discount. There are myriad factors that went into insurer B getting that lower price. Insurer B might have a disproportionate share of the patients needing that procedure in that region, and in exchange for funneling their patients to the hospital in question rather than a competing hospital, they received a lower per-patient price. But once the prices are all public, sooner or later the prices will equalize. It’s not guaranteed, however, or even likely, that the lowest price previously available will be the one that the market settles on. Shining light on the various discounts insurers negotiate is more likely to lead to fewer discounts than to more people getting them. With perfect knowledge comes perfect pricing, but perfect pricing isn’t necessarily cheaper pricing.
Chart Review
Kate Dixon, Health Care Policy Intern
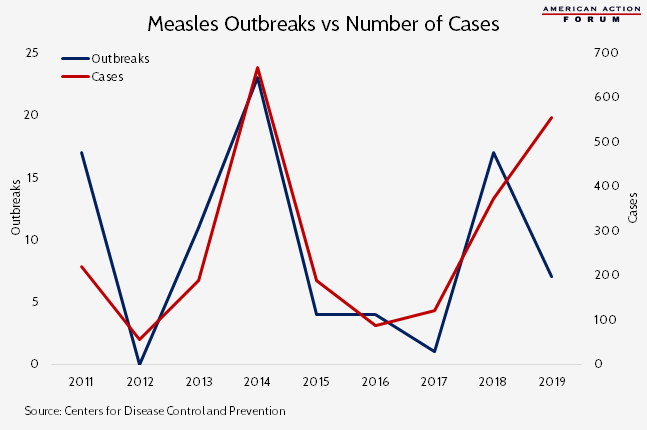
Recently, following a large spike in measles infections in New York City, Mayor de Blasio declared a public health emergency requiring all unvaccinated individuals in Brooklyn to receive the measles vaccine. The NYC outbreak (with “outbreak” defined as 3 or more linked cases in an area) is one of six currently ongoing in 2019 (with a seventh, in Texas, no longer listed as ongoing on CDC’s website). As of April 11, the country has seen 555 cases just this year, already more cases than any other year since 2000 with the exception of 2014. Between 2009-2014, the median number of cases per outbreak was 5, while in 2015 (excluding the Disneyland outbreak accounting for 78 percent of 2015 cases) the average number of cases per outbreak was 9. Historically, the number of total cases has been highly correlated with the number of outbreaks. This year, however, fewer outbreaks are accounting for a greater number of cases, indicating greater difficulty at containment of the disease: 5 of the 7 outbreaks this year have been associated with more than 10 cases each.
Team Health Around Town
Health Affairs: The Implications Of Recalibrating Medicare Advantage Risk Adjustment Using Encounter Data
AAF President Douglas Holtz-Eakin and Christopher Holt co-authored a post examining the implications of adjusting Medicare Advantage’s capitated payment using patient data from Medicare Advantage itself.
AEI Event: Medicare’s perilous fiscal future – The 2019 Trustees Report
Deputy Director of Health Care Policy Tara O’Neill Hayes will discuss the fiscal future of Medicare at the American Enterprise Institute on Tuesday, April 23rd.
