







Insight
March 8, 2023
Justice Department Withdraws Health Care Antitrust Enforcement Policy Statements
Executive Summary
- On February 3, 2023, the Department of Justice (DOJ) withdrew three decades-old policy statements that established antitrust safety zones, which provide circumstances under which the antitrust enforcement agencies will not challenge certain activity, in health care markets.
- The agency claimed the guidance statements no longer reflected a “significantly changed healthcare landscape” and were “overly permissive on certain subjects, such as information sharing.”
- While the DOJ pointed to “recent enforcement actions and competition advocacy” as a replacement, this approach is insufficient as guidance for health care industry participants: The withdrawn guidance informed past precedents, and without it, the health care industry will have to wait for future antitrust action to understand the DOJ’s enforcement policy; this uncertainty could result in fewer collaborative efforts that accelerate the adoption of new technologies and lower costs.
Introduction
The Department of Justice (DOJ) withdrew three decades-old policy statements that provided insight into the agency’s antitrust enforcement approach in health care markets on February 3, 2023. The withdrawal leaves hospitals and other industry participants without clear guidance as to what business activities are permissible under antitrust law. The policy statements were jointly issued by the DOJ and the Federal Trade Commission (FTC), but the FTC has yet to independently withdraw the guidance, sowing further confusion.
The DOJ asserted that the policy statements were outdated and did not adequately reflect the significantly changed health care market landscape.
The statements established antitrust safety zones, circumstances under which the antitrust enforcement agencies will not challenge certain activity, for information exchanges, hospital mergers, joint ventures, and Accountable Care Organizations (ACO) participating in the Medicare Shared Savings Program (MSSP) covering millions of patients.
The DOJ advised that industry participants should consult “recent enforcement actions and competition advocacy” as a replacement. This is insufficient: The withdrawn guidance informed past precedents, and without it, the health care industry will have to wait for future antitrust action to understand the DOJ’s enforcement policy. This uncertainty could result in fewer collaborative efforts that accelerate the adoption of new technologies and lower costs. The withdrawal also leaves current arrangements vulnerable to increased antitrust enforcement.
DOJ Statement
On Feb. 3, 2023, the DOJ’s Antitrust Division withdrew three policy statements related to enforcement in health care markets: Antitrust Enforcement Policy Statements Issued for Health Care Industry (1993), Statements of Antitrust Enforcement Policy in Health Care (1996), and Statement of Antitrust Enforcement Policy Regarding Accountable Care Organizations Participating in the Medicare Share Savings Program (2011).
While policy statements are not legally binding, they provide crucial information with respect to how the antitrust enforcement agencies consider certain business activities. The three policy statements established antitrust safety zones, which outline criteria for the health care industry to avoid antitrust scrutiny.
The DOJ claimed that the health care industry has changed significantly since the first of the now-withdrawn policy statements, which the agency called “outdated,” was issued in 1993. Assistant Attorney General of the Antitrust Division Jonathan Kanter added that the decision was “long overdue.” The agency asserted the guidance documents “no longer serve their intended purpose of providing encompassing guidance to the public on relevant healthcare competition issues,” and that they were “overly permissive on certain subjects, such as information sharing….”
In lieu of a replacement policy, the DOJ stated that “[r]ecent enforcement actions and competition advocacy in healthcare provide guidance to the public….” Yet businesses will have difficulty using recent enforcement actions because any prior DOJ investigations and actions were guided by policies outlined in the various statements. Without clear guidance from the DOJ on which participants in the health care industry can rely, they will only be able to evaluate how the DOJ will approach antitrust enforcement based on the agency’s future actions, leaving the industry unable to alter current activity with certainty.
Information Exchanges
Principal Deputy Assistant Attorney General Doha Mekki of the DOJ’s Antitrust Division delivered a speech announcing the withdrawal of the three policy statements and discussed the difficulty of antitrust safety zones for information exchanges, asserting that exchanging competitively sensitive information could “[facilitate] price or wage fixing, bid rigging, or market allocation….”
Information exchanges are surveys of competing providers that include data on the prices charged for health care services, salaries, wages, and other benefits. Such information allows a company to gauge its competitiveness. Information exchanges, without safeguards, could “facilitate collusion or otherwise reduce competition on price or competition….” The 1993 statement, updated with changes in 1996, outlined these safeguards and established antitrust safety zones for information exchanges. The terms of a lawful information exchange included: 1) the survey is managed by a third party; 2) the information provided by survey participants is based on data more than three months old; and 3) there are at least five providers reporting data upon which each disseminated statistic is based, no individual provider’s data represents more than 25 percent on a weighted basis of that statistic, and any information disseminated is sufficiently aggregated such that it would not allow recipients to identity the prices charged or compensation paid by any particular provider.
Mekki stated, referring to these information exchanges, that the “safety zones were written at a time when information was shared in manila envelopes and through fax machines. Today, data is shared, analyzed, and used in ways that would be unrecognizable decades ago.”
Mekki’s explanation of the DOJ’s pivot and the withdrawal of the policy statements leave current information exchange programs exposed to heightened antitrust enforcement and likely limit the formation of new exchanges.
Mergers
Concern over hospital consolidation was a centerpiece of President Biden’s 2021 executive order on Promoting Competition in the American Economy, which asserted that “hospital consolidation has left many areas, particularly rural communities, with inadequate or more expensive healthcare options.”
The 1993 policy statement provided an antitrust safety zone with respect to mergers for small hospitals. The policy statements hold that, as a condition of the safety zone, “[a] merger in which one of the merging hospitals has less than 100 licensed beds and an average daily inpatient census of less than 40 patients” will not be challenged absent extraordinary circumstances. Additional qualifiers regarding the safety zone were added in the 1996 policy statement.
Data seen in Figure 1 show that more than 3,400 hospitals, over 56 percent, had fewer than 100 beds in 2022. Limiting the data to community hospitals – which include all non-federal, short-term general, and special hospitals whose facilities and services are available to the public – tells a similar story, as shown in Figure 2. Nearly 57 percent of all community hospitals had fewer than 100 beds in 2020, with 52 percent located in rural areas. Some of these rural hospitals were likely operating in the antitrust safety zone if involved in a merger, but the removed guidance leaves those hospitals vulnerable to increased antitrust enforcement.
Figure 1
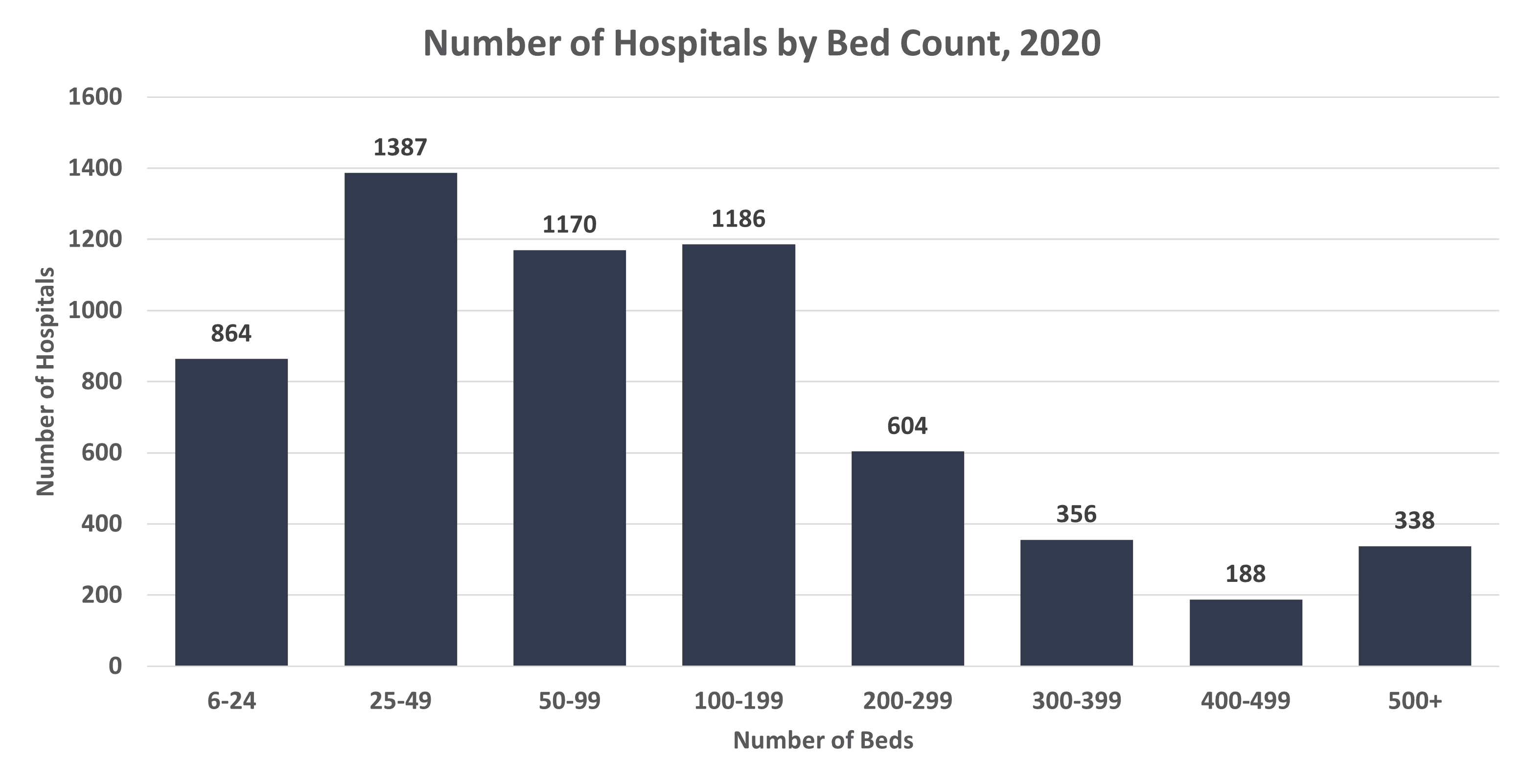
*Data source: American Hospital Association
Figure 2
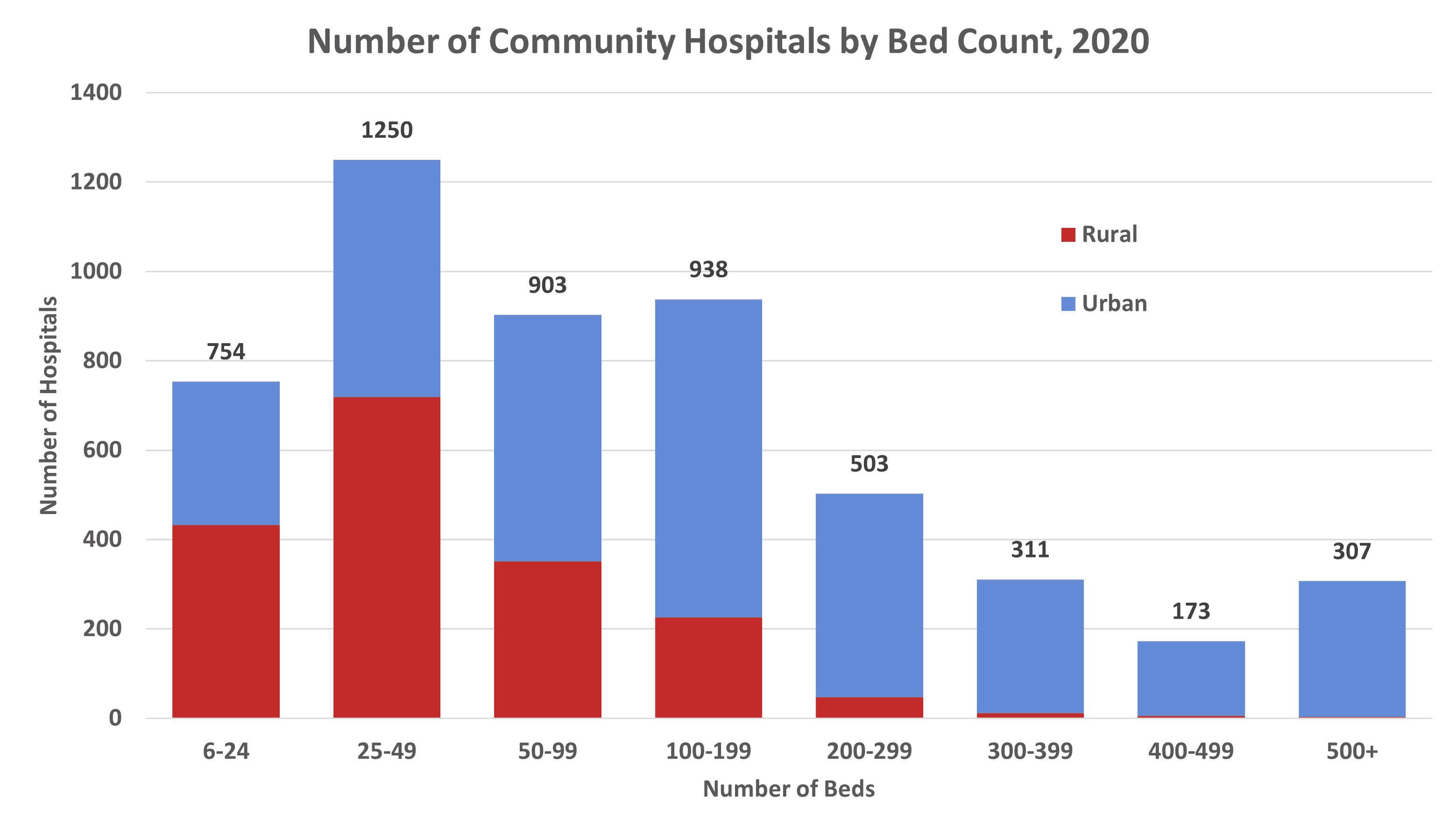
*Data source: American Hospital Association
The 1996 guidance notes that small hospitals merging with a larger hospital could result in cost-saving efficiencies and present little risk to competition. For example, a hospital with fewer than 100 licensed beds and a daily inpatient census of fewer than 40 patients may be the only hospital in the relevant market, and thus unlikely to “compete in any significant way with other hospitals…[and] are unlikely to reduce competition substantially,” according to the policy statement.
Joint Ventures Involving High-cost Equipment
High-cost equipment such as MRI machines and PET/CT scanners can be prohibitively expensive for a single hospital to acquire and operate, particularly in rural areas. The 1993 policy statement created an antitrust safety zone for joint ventures involving the purchase and operation of such equipment.
The antitrust agencies acknowledged in the policy statement that “[a]lthough numerous hospitals presently participate in joint ventures, it has been suggested that fear of antitrust enforcement currently chills such ventures and forces hospitals to purchase expensive equipment individually, even though joint ventures clearly would be more efficient and less expensive.” The statement made clear that only hospitals that cannot independently purchase or operate the equipment can be included in the agreement.
By assuring hospitals that such conduct, barring extraordinary circumstances, would not face antitrust action, it is likely that these joint ventures successfully expanded the availability of procedures involving MRI, PET/CT, and other expensive medical equipment. These joint ventures also facilitate the adoption of new, expensive technologies that would otherwise be cost prohibitive to an individual hospital.
The policy statement issued in 1996 reaffirmed the antitrust agencies’ stance on joint ventures, adding some qualifying statements to the antitrust safety zones. The withdrawal of the policy statement will likely hinder the creation of new joint ventures involving high-cost equipment and leave current agreements susceptible to increased enforcement, all while delaying the deployment of new technologies.
Accountable Care Organizations
The Affordable Care Act created the Medicare Shared Savings program, designed to promote accountability for a given patient population, coordinate items and services for Medicare fee-for-service beneficiaries, and encourage investment in high quality and efficient services. MSSP leveraged accountable care organizations, which are groups of doctors, hospitals, and other health care providers working together to coordinate patient care. The 2011 policy statement established clearly defined ACO antitrust safety zones.
According to the Centers for Medicare and Medicaid Services, there were 220 ACOs serving 3.2 million assigned beneficiaries in 2012 and 2013. After the number of ACOs peaked in 2018 at 561, there were 456 in January 2023 with 10.9 million assigned beneficiaries.
Sharing costs and other financial information among care providers is a necessary function of ACOs, and the 2011 policy statement included clear guidance of activities it would consider unlawful. Without the policy statement, as well as the DOJ’s claim that its previous protection of information sharing was “overly permissive,” the effectiveness of ACOs to provide coordinated, cost-effective care may be reduced, as participants will lack clarity as to whether current information sharing practices are considered unlawful.
Conclusion
The DOJ’s withdrawal of the three policy statements that established antitrust safety zones in health care markets will sow deep uncertainty among providers, hospitals, and other industry participants. While it is possible the DOJ’s antitrust approach on some of these safety zones will remain unchanged, it will be difficult for participants in the health care industry to know with any level of certainty.
Merely pointing to recent enforcement actions and competition advocacy as a replacement for clear and authoritative policy sources will be insufficient for the DOJ to maintain certainty in the health care industry. Collectively, these actions will likely throw cold water on new collaborative efforts and leave current arrangements vulnerable to increased antitrust scrutiny.
