







Insight
September 27, 2022
FTC Warns That Monopoly Hospitals Use State COPA Laws to Evade Antitrust Enforcement
Executive Summary
- Currently, 19 states have some version of Certificate of Public Advantage (COPA) laws, which permit hospitals in a concentrated market to merge if the state believes the likely benefits outweigh the potential harms from a loss of competition and shield the merger from federal antitrust enforcement.
- The Federal Trade Commission recently warned that substituting market competition with regulatory oversight using COPA laws is insufficient to protect consumers.
- A lack of resources, regulatory fatigue, and the repeal of COPA laws post-merger prevents states from ensuring hospital monopolies cannot leverage market power in the form of higher prices and reduced quality of care over the long term.
- Several COPA case studies showed that inpatient prices in the years immediately following COPA increased at least 20 percent, and between 39 percent and 51 percent after the repeal or expiration of the state regulation.
Introduction
The Federal Trade Commission (FTC) recently warned states against the use of Certificate of Public Advantage (COPA) laws, which allow hospitals in concentrated markets to merge if the state believes the likely benefits outweigh the potential harms. These laws substitute market competition with state regulatory oversight and shield mergers from federal antitrust enforcement under the state action doctrine, which shields certain state regulatory actions from antitrust scrutiny.
The Federal Trade Commission (FTC) “routinely challenges hospital mergers that would substantially lessen competition, and therefore would raise healthcare prices for patients, reduce quality of care, [and] limit access to healthcare services….”
Currently, 19 states have some version of a COPA law, and FTC research found that nine states have approved hospital mergers using them. Although the use of COPA is rare, the merger often leads to undesirable outcomes including higher prices and less health care access for patients.
It is often the case that, over time, states in which hospitals merged using COPA lack resources and suffer regulatory fatigue. These factors limit states’ ability to provide the necessary oversight to prevent a monopoly hospital from exercising its market power.
A more dire outcome occurs when states have repealed COPA laws long after a merger has been completed. The FTC found that three states, North Carolina, Montana, and Minnesota, repealed COPA legislation following a merger. The repeal removed all the COPA protections and oversight, leaving hospitals free to exert their unconstrained market dominance.
In the recent FTC policy paper, the agency “advocat[ed] against the use of COPAs to shield otherwise illegal hospital mergers.” It also urged “states that have existing COPA laws to consider repealing those laws if they do not have an active COPA in place.”
States that adjust policy based on the FTC recommendations are likely to restore competitive markets, remove barriers to antitrust enforcement, and protect patients from substantial price increases.
COPA Laws
COPA laws “allow hospitals to merge if [the state] determine[s] the likely benefits from a particular merger outweigh any disadvantages from reduced competition and increased consolidation.” These laws generally include conditions on the COPA recipient including “price controls and rate regulations, mechanisms for sharing cost savings and efficiencies, and commitments about certain contraction provisions between hospitals and commercial health insurers.”
COPA laws also shield the otherwise illegal merger and other activities from federal antitrust enforcement if the state perceived the benefits would outweigh the cost of lost competition.
Currently, 19 states have some version of a COPA law, with the most recent being enacted in Indiana in 2021. Figure 1 is a map published by The Source on Healthcare Price & Competition depicting the COPA law landscape.
Figure 1

State Action Doctrine
The FTC cited the state action doctrine as limiting factor in challenging a merger under COPA. The agency explained that the state action doctrine “emerged in response to efforts to apply antitrust rules to the activities of state governments, and is rooted in the notion that Congress passed the Sherman Act to protect competition, not to limit the sovereign regulatory powers of the states.
The state action doctrine “shield[s] certain regulatory conduct from federal antitrust enforcement, provided that the conduct is: 1) furtherance of a clearly articulated state policy, and 2) actively supervised by the state.”
A COPA law that complies with these conditions would limit the FTC’s ability to challenge the merger.
The FTC admitted that in cases where COPA laws are repealed and, consequently, the state action doctrine no longer applies, “antitrust enforcement was no longer practical since the mergers had long been consummated.”
Hospital Concentration
The market structure for inpatient hospital services is highly concentrated, in part because of the role geography plays relative to other goods and services. The National Law Review discovered that “[m]arkets for inpatient hospital services are generally considered to be geographically compact. Patients are unwilling to travel far for certain services, so providers separated by long distances are considered unlikely to compete with each other.” This condition limits potential competition among hospitals.
Pew Research Center found that the average commuting time to the closest hospital ranges from 11.7 minutes in the Middle Atlantic region to 15.8 minutes in the West North Central region. A map of the commuting times is displayed in Figure 2.
Figure 2
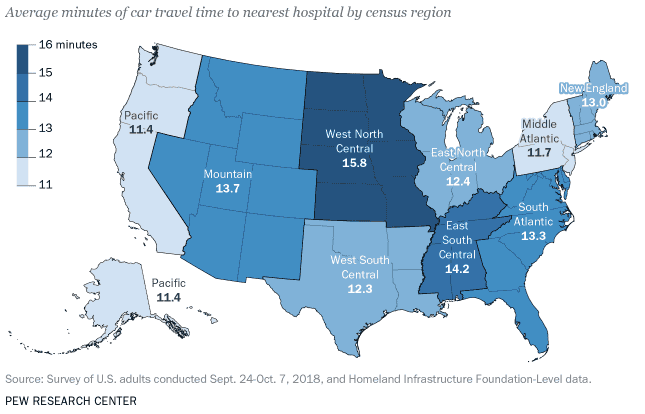
Because the geographical range of hospital market services is limited, a hospital operating outside the current commuting average may not be a viable competitor.
To help illustrate the structural challenges in the hospital market, Health Care Cost Institute published the Hospital Concentration Index data set. The data showed that “In 2020, 125 metros of the 186 studied (67 percent) had hospital markets that were highly or very highly concentrated based on their [Herfindahl-Hirschman Index (HHI)] level.”
Figure 3 shows the distribution of hospital concentration in 2020. Each rectangle represents a different metro area and is color coded based on the 2020 HHI.
Figure 3
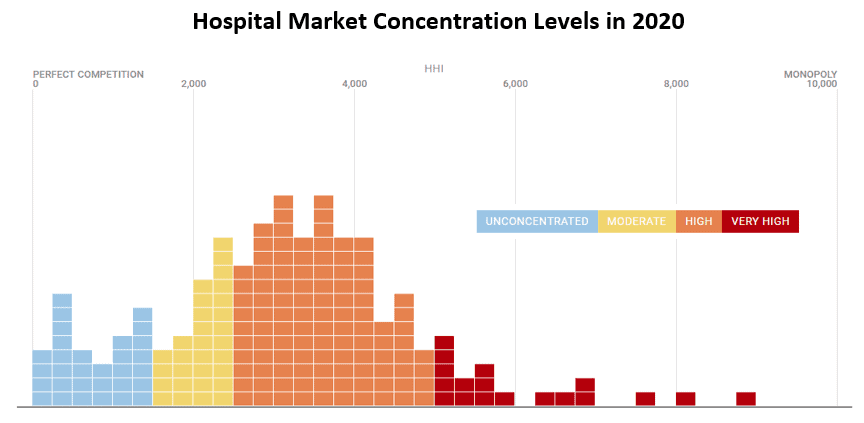
*Data taken from Health Care Cost Institute Hospital Concentration Index
The Horizontal Merger Guidelines (HMG) jointly published by the FTC and the Department of Justice state that mergers that result in moderately or highly concentrated markets raise competitive concerns. In a highly concentrated market, an “increase in the HHI of more than 200 points will be presumed to be likely to enhance market power.”
The FTC’s warning against the use of COPA reflects the current market structure. Hospital mergers within a metro area where the market is already highly concentrated are almost certain to raise antitrust concerns based on the criteria outlined in the HMG. A state that entered into an agreement under the COPA law limits the FTC’s ability to challenge it, however.
Case Studies on the Effects of COPA Laws
The FTC policy paper warning states against the use of COPA laws included several case studies showing the ineffectiveness of COPA laws in controlling health care costs and quality of care.
The study of the Mission Health COPA in North Carolina found “substantial increases in commercial inpatient prices during early COPA years (at least 20%) …. [a]nd even greater price increases after the COPA was repealed (at least 38%).”
The results of this case study, and others provided by the FTC, include ample evidence that price regulations put in place using COPA were ineffective. The findings also highlighted the risk an unregulated monopoly can have on prices following a COPA repeal.
A recent article from health news company STAT offered further evidence of such price increases. The article cited a study slated to appear in the Journal of Law and Economics that concluded hospitals “hiked prices between 39% and 51% after the repeal or expiration of their state regulated [COPA].”
Conclusion
COPA laws permit hospitals in a concentrated market to merge and shield the merger from federal antitrust enforcement.
Several studies quantified COPA’s lack of success in preventing inpatient price increases. In the years immediately following a COPA merger, inpatient prices increased at least 20 percent. Similarly damaging were the price hikes between 39 percent and 51 percent that followed the repeal or expiration of a state COPA regulation.
The FTC warned that a lack of state resources, regulatory fatigue, and even the repeal of COPA laws post-merger reduces the state’s ability to ensure hospital monopolies cannot leverage market power. The agency asserted that attempting to substitute market competition among hospitals with regulatory oversight will, over time, prove ineffective at preventing increased prices or decreased quality of care.
