







Weekly Checkup
October 4, 2024
CMS’ New Gene Therapy Model Has Cost-saving Promise
The Centers for Medicare and Medicaid Services (CMS) recently confirmed it would be rolling out a new access model for novel sickle cell disease (SCD) gene therapy treatments to help patients on state Medicaid programs. Let’s discuss how this model could improve health outcomes for those with SCD and treat them at a lower lifetime cost.
For context, SCD is a collection of inherited genetic disorders that alters how the body interacts with hemoglobin. In a person without SCD, hemoglobin (which is exclusively found in red blood cells) latches onto oxygen and carbon dioxide, enabling red blood cells to transport these components throughout the body and respiratory cycle. Among those with SCD, the body produces an abnormal form of hemoglobin known as Hemoglobin S, which renders the red blood cells more rigid and causes them to take on a sickle shape. The condition carries with it a host of life-threatening complications, including an increased susceptibility to blood clots, infections, acute chest syndrome, and splenic sequestration.
CMS’ model, the Cell and Gene Therapy (CGT) Access Model, is a new approach by the Biden Administration to reduce the cost of treating patients’ SCD over their lifetime by taking advantage of new gene therapy innovations that allow doctors to halt the progression of SCD, effectively curing patients. By negotiating directly with manufacturers (on behalf of Medicaid plans), CMS aims to establish an outcome-based payment framework that allows for lower SCD gene therapy treatment costs for states and ties manufacturer payments to improved patient health outcomes. Should the CGT model prove effective, CMS has signaled it may expand the model to include other conditions.
There are currently two Food and Drug Administration-approved gene therapy treatments on the market, with costs hovering between roughly $2–3 million per patient – and these treatment costs don’t include several additional therapies patients are required to undergo both before and during treatment. Put simply, these gene therapies are incredibly expensive, but when compared to the lifetime burden of total medical costs attributable to SCD among nonelderly individuals with commercial insurance (approximately $1.7 million with an associated out-of-pocket cost of roughly $44,000), these costs don’t appear as outlandish. Should CMS’ model succeed in negotiating gene therapy prices closer to or even marginally lower than the lifetime burden of medical costs attributable to SCD among nonelderly individuals, it is conceivable that it would be more cost effective to cure participating states’ Medicaid enrollees of SCD rather than simply treating SCD’s associated symptoms.
The CGT model could be an important advancement for the future of preventive health care in the United States if CMS can appropriately implement its model. This will require both using state Medicaid negotiating power to lower prices through bundled purchasing and refraining from meddling in the market with price controls and closed-door negotiations (akin to those used in the Inflation Reduction Act drug negations). If CMS does this, the CGT model could be a promising avenue for many Medicaid enrollees to receive curative care for genetic disorders and a potential saver for the federal government.
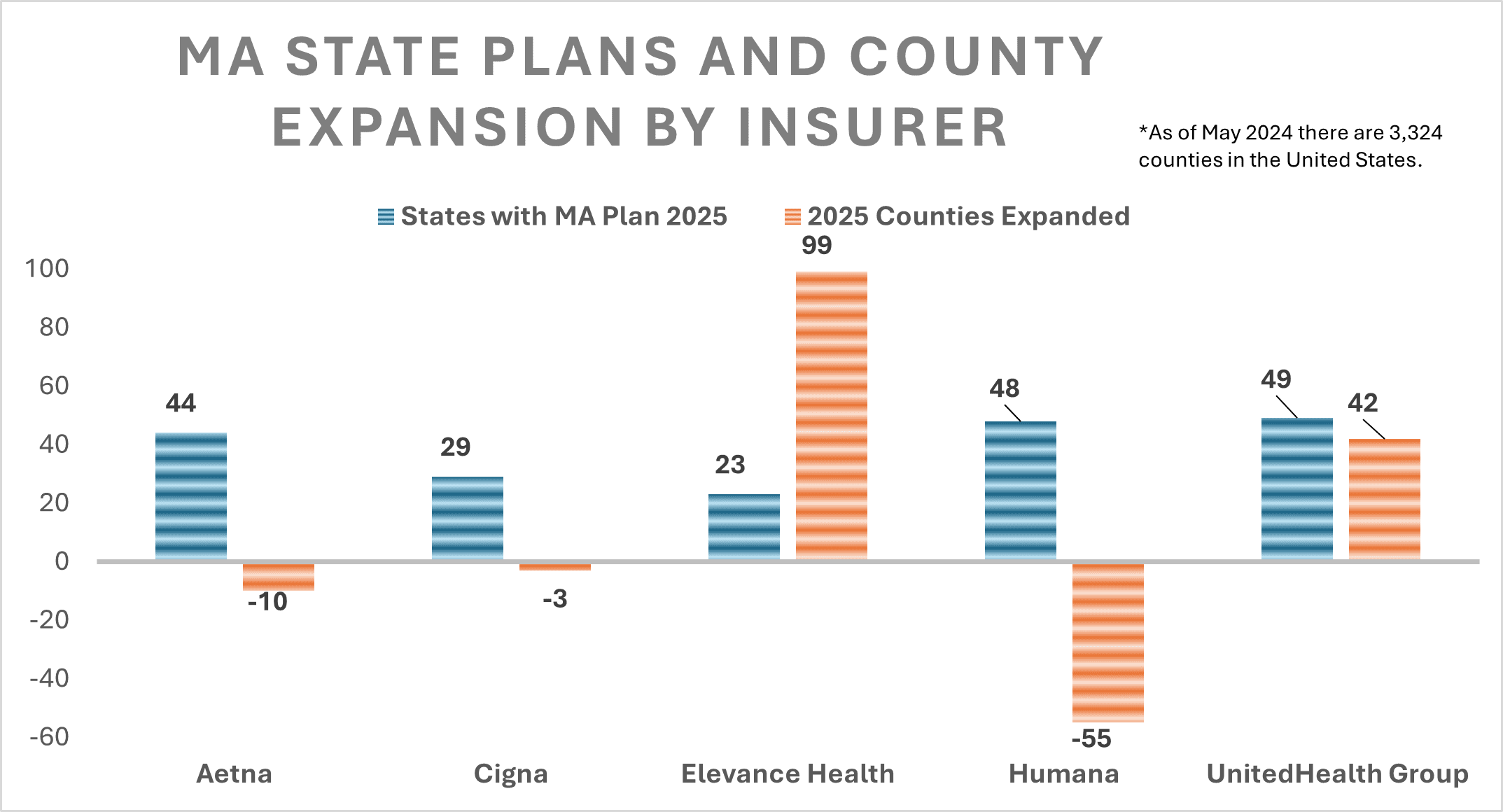
Medicare Advantage Expansion Report Shows Mixed Results for 2025 Coverage
Parth Dahima, Health Care Data Analyst
Five leading health insurers launched their Medicare offerings for fiscal year 2025, giving consumers a glimpse at expansions and reductions in coverage. Due to new measures included in the Centers for Medicare and Medicaid’s Medicare Advantage (MA) Star Ratings data, insurers projected various changes in their profitability, driving them to make changes to their county coverage, and some total state coverage. Moreover, most made moderate modifications to the composition of their offerings.
Elevance Health and UnitedHealth announced moderate expansions of their MA footprint, adding 99 and 42 counties to their respective MA plans. Conversely, Aetna, Humana, and Cigna announced reductions in counties served. Yet the five insurers project only minimal changes to the total states in which they offer MA plans. The graph below illustrates the number of states in which the five largest insurers operate, as well as the net change in counties served between fiscal years 2024 and 2025. Of note is the net change in total U.S. counties served in 2025 – a 73-county increase from 2024.
Sources:
https://www.healthcare-economist.com/2024/09/26/what-are-the-new-cms-star-ratings-measures-for-2025/#:~:text=The%20CMS%20Star%20Ratings%20are%20very%20important%20as%20CMS%20payments
https://newsroom.cigna.com/cigna-healthcare-medicare-2025-plans

